

Safety Training Seminars

The Pediatric Cardiac Arrest Algorithm following AHA 2025 Guidelines delivers a comprehensive, evidence-based approach for managing pediatric cardiac arrest. Learn high-quality CPR priorities, rhythm-specific interventions, airway management, medication dosing, and post-resuscitation care to optimize survival, neurological outcomes, and overall pediatric emergency response effectiveness.
When a child’s heart stops beating, every second counts. The pediatric cardiac arrest algorithm provides healthcare providers with a systematic approach to resuscitate young patients effectively. This evidence-based protocol can mean the difference between life and death for children experiencing cardiac emergencies.
Healthcare professionals who work with pediatric patients must understand this algorithm inside and out. Whether you’re a nurse, physician, or emergency responder, mastering these steps will prepare you to act quickly and confidently when facing one of medicine’s most critical situations.
The pediatric cardiac arrest algorithm follows specific guidelines developed by the American Heart Association. These protocols have been refined through years of research and real-world application, giving medical teams the best chance of achieving successful outcomes.
The Pediatric Cardiac Arrest Algorithm is a systematic guide developed by organizations like the American Heart Association (AHA) for managing cardiac arrest in infants and children. It prioritizes high-quality CPR and identifies the underlying cause of the arrest to guide treatment.
The algorithm is split into two main pathways based on the child’s heart rhythm:
Promptly identifying the rhythm is crucial, as it determines whether defibrillation is needed.
Regardless of the specific rhythm, the foundation of the Pediatric Cardiac Arrest Algorithm is built on several key actions. These must be performed quickly and efficiently.
As soon as you recognize a child is in cardiac arrest, start CPR. This is the single most important intervention. High-quality CPR for children involves:
The compression-to-ventilation ratio is 30:2 for a single rescuer and 15:2 for two rescuers.
While CPR is in progress, another team member should attach a monitor or defibrillator to the child. This allows for a quick rhythm check to determine if the rhythm is shockable or non-shockable. This analysis should happen during a brief pause in compressions, ideally lasting no more than 10 seconds.
If the rhythm check reveals Ventricular Fibrillation (VF) or pulseless Ventricular Tachycardia (pVT), the immediate action is to deliver a shock.
The recommended initial energy dose for defibrillation in children is 2 joules per kilogram (J/kg) of the child’s weight. If a second shock is needed, the dose can be increased to 4 J/kg. Subsequent shocks can be administered at doses up to 10 J/kg or the maximum adult dose.
As soon as the shock is delivered, resume high-quality CPR for two minutes. Do not pause to check for a pulse right away. The goal is to maximize blood flow to the brain and other vital organs.
If the child remains in cardiac arrest after the first two minutes of CPR post-shock, establish IV or IO (intraosseous) access. Administer epinephrine every 3 to 5 minutes. Epinephrine helps constrict blood vessels, increasing blood pressure and blood flow to the heart.
After the second shock, you may consider placing an advanced airway, such as an endotracheal tube. If VF or pVT persists, administering an antiarrhythmic medication like Amiodarone or Lidocaine may be necessary. These medications can help stabilize the heart’s rhythm.
Continue this cycle of CPR, rhythm checks, shocks, and medication until the child achieves Return of Spontaneous Circulation (ROSC) or resuscitation efforts are stopped.
If the rhythm check shows Asystole (a flat line) or Pulseless Electrical Activity (PEA), the approach is different because shocks are not effective.
For non-shockable rhythms, the priority is to administer epinephrine as soon as IV/IO access is available. Continue giving it every 3 to 5 minutes throughout the resuscitation effort.
Resume CPR immediately after the rhythm check. Since defibrillation is not an option, continuous, high-quality CPR is the primary treatment. The cycle remains two minutes of CPR followed by a rhythm check.
While performing CPR, it is vital to search for and treat any reversible causes of the cardiac arrest. These are often remembered by the “H’s and T’s”:
Addressing these underlying issues is often the key to achieving ROSC in cases of Asystole or PEA.
If the team successfully achieves ROSC, the work is not over. Post-cardiac arrest care is critical for improving the child’s chances of a good outcome. This includes optimizing ventilation and oxygenation, treating hypotension, and managing the child’s temperature to protect the brain.
Reading about the Pediatric Cardiac Arrest Algorithm is a great first step, but true competence comes from hands-on practice. At Safety Training Seminars, we offer American Heart Association (AHA) Pediatric Advanced Life Support (PALS) courses designed for healthcare professionals. Our PALS certification program combines a flexible online course with a brief, in-person skills session.
In our training, you will use voice-assisted manikins to practice high-quality CPR and run realistic scenarios. This approach helps build the muscle memory and confidence needed to act decisively in a real emergency. With over 70 locations throughout California, we make it convenient to get the certification you need. We guarantee the lowest prices and provide your AHA certification card on the same day you complete your training. Book an appointment today and be prepared to save a life.
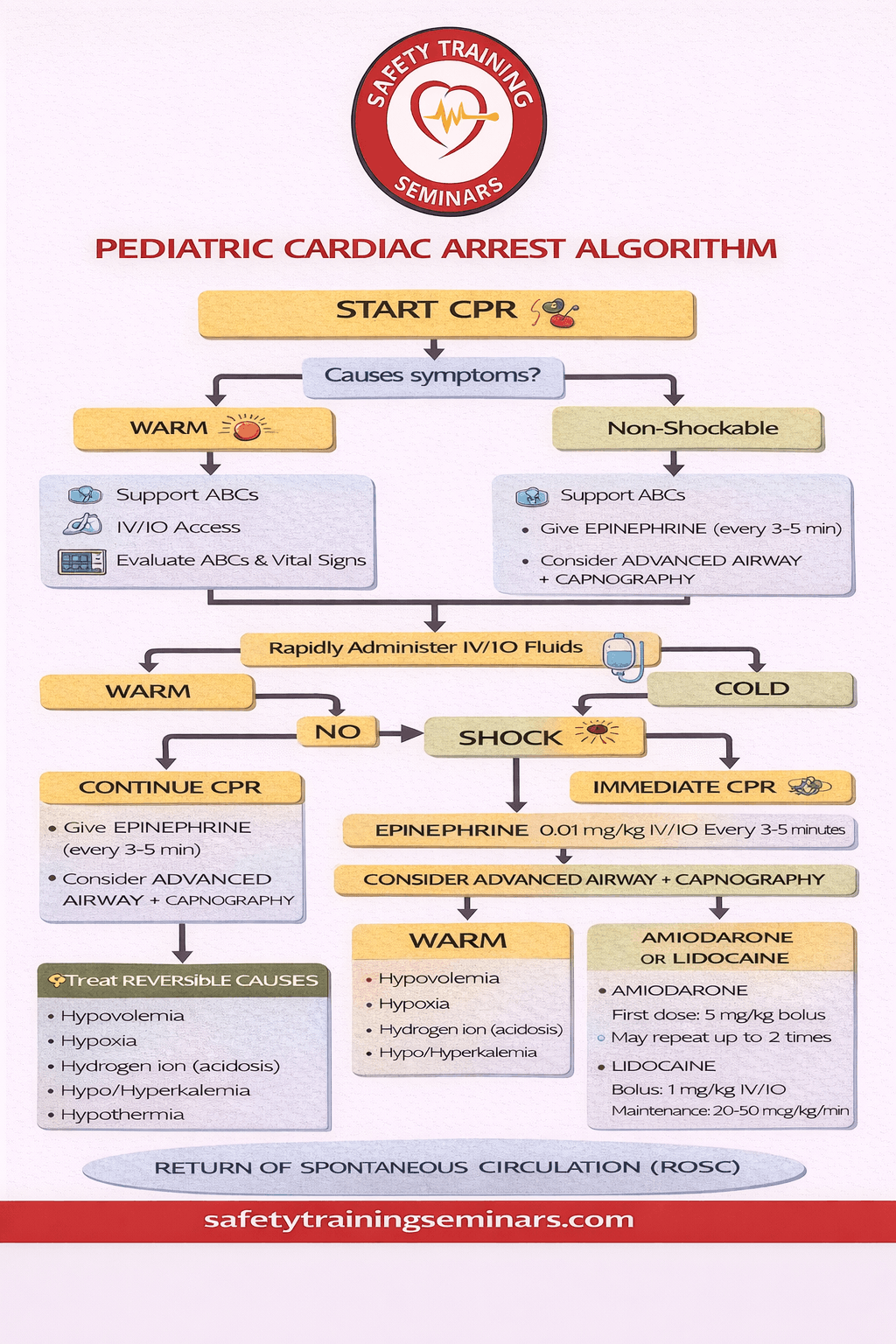
The Pediatric Cardiac Arrest Algorithm is a vital tool for healthcare professionals, first responders, and caregivers to effectively manage life-threatening cardiac emergencies in children. This infographic provides a clear, step-by-step visual representation of pediatric resuscitation, emphasizing rapid recognition of cardiac arrest signs. Early identification—such as unresponsiveness, abnormal breathing, or absent pulse—is critical for activating emergency medical services and starting immediate life-saving interventions. By following the algorithm, responders can ensure timely CPR and prepare for defibrillation with pediatric-appropriate protocols.
Central to the algorithm is high-quality pediatric resuscitation. The infographic breaks down the correct techniques for chest compressions, ventilation, and the use of automated external defibrillators (AEDs) adapted for infants and children. It also guides healthcare providers on administering essential medications, like epinephrine, and addressing reversible causes of arrest, including respiratory failure, hypovolemia, or electrolyte imbalances. By presenting these procedures in a structured, visual format, the algorithm enables rapid decision-making during high-stress situations, improving survival outcomes.
The final component focuses on post-resuscitation care and monitoring. After the return of spontaneous circulation (ROSC), ongoing assessment of vital signs, oxygenation, and neurological function is essential to prevent complications. This infographic simplifies complex pediatric cardiac protocols, making them accessible and actionable for medical professionals. Adhering to the Pediatric Cardiac Arrest Algorithm ensures not only effective resuscitation but also better long-term recovery for children experiencing cardiac emergencies.
The pediatric cardiac arrest algorithm provides a structured approach to recognizing and managing cardiac arrest in children. It guides healthcare providers through CPR, defibrillation, and advanced life support interventions to improve survival and neurological outcomes.
In children, cardiac arrest is often secondary to respiratory failure or shock rather than primary cardiac causes. The algorithm emphasizes airway management, ventilation, high-quality CPR, and early recognition of reversible causes specific to pediatric patients.
Defibrillation is indicated for shockable rhythms such as ventricular fibrillation or pulseless ventricular tachycardia. Early defibrillation combined with CPR significantly increases the chances of survival and reduces the risk of long-term neurological complications.
After Return of Spontaneous Circulation (ROSC), focus shifts to stabilizing airway, circulation, and neurological function. Continuous monitoring, oxygen therapy, temperature management, and treatment of the underlying cause are critical for recovery.
Yes, emergency responders can apply the algorithm during out-of-hospital emergencies. Following these steps ensures timely CPR, defibrillation, and rapid transport to a hospital, increasing survival rates for children experiencing cardiac arrest.