

Safety Training Seminars

The Cardiac Arrest in Pregnancy In-Hospital ACLS Algorithm based on AHA 2025 Guidelines outlines specialized, life-saving modifications for maternal resuscitation. Learn key updates on left uterine displacement, airway management, medication use, defibrillation safety, and perimortem cesarean delivery to optimize outcomes for both mother and fetus.
Cardiac arrest during pregnancy is a rare but critical emergency. When it happens, healthcare providers must act fast. They need to manage two patients at once: the mother and the fetus. The standard Advanced Cardiovascular Life Support (ACLS) protocol needs adjustments to improve outcomes for both.
Understanding this modified approach is essential for any healthcare professional in an acute care setting. It involves specific techniques and considerations that address the unique physiological changes of pregnancy. Knowing these steps helps ensure the resuscitation team can provide the best possible care during a high-stakes emergency. This post will walk you through the key components of the algorithm, from manual uterine displacement to the timing of a perimortem cesarean delivery.
When a pregnant patient goes into cardiac arrest, the standard ACLS guidelines are the foundation of care. However, the team must immediately implement maternal-specific modifications. The primary goal is to relieve the physiological burdens of pregnancy that can interfere with resuscitation.
The algorithm runs parallel to the standard ACLS sequence of chest compressions, airway management, and defibrillation. The key is to integrate maternal interventions without delaying standard lifesaving care. A designated team leader should assign roles quickly, ensuring one person is responsible for maternal-specific tasks while others manage the primary cardiac arrest response.
The moment cardiac arrest is identified in a pregnant patient, the resuscitation team should initiate the following actions simultaneously with high-quality CPR:
While the core principles of ACLS remain, several adjustments are necessary to optimize the resuscitation of a pregnant patient. These changes account for the anatomical and physiological shifts that occur during pregnancy.
Continuous, high-quality chest compressions are vital. For pregnant patients, compressions should be performed slightly higher on the sternum to account for the elevation of the diaphragm.
Throughout the resuscitation, Manual Uterine Displacement must be maintained. If MUD is not effective or feasible, the team can place the patient in a 30-degree left lateral tilt using a wedge or pillows. However, MUD is preferred because it allows the patient to remain supine, which makes high-quality chest compressions easier to perform.
Because of increased aspiration risk and potential difficulty with intubation, experienced personnel should manage the airway. A smaller endotracheal tube may be necessary due to airway edema. Continuous waveform capnography is essential to confirm tube placement and monitor CPR quality.
The indications and energy doses for defibrillation are the same for pregnant patients as for non-pregnant patients. There is no evidence that defibrillation harms the fetus.
Similarly, standard ACLS drug protocols, including epinephrine and amiodarone, should be followed without modification. The priority is maternal survival, which offers the best chance for fetal survival.
If the patient does not achieve Return of Spontaneous Circulation (ROSC) quickly, the team must prepare for a perimortem cesarean delivery. This procedure is also known as a resuscitative hysterotomy.
The goal of a PMCD is twofold:
The decision to perform a PMCD should be made rapidly. The “four-minute rule” is a critical guideline: if there is no maternal ROSC within four minutes of the cardiac arrest, the team should begin the cesarean delivery. The goal is to deliver the baby by the fifth minute.
This timeline is crucial because the chances of both maternal and fetal survival decrease significantly as time passes. The delivery should occur at the site of the arrest, whether it’s in the emergency department, ICU, or operating room. Do not move the patient. The procedure must be performed while high-quality CPR and other ACLS interventions continue.
Identifying and treating the underlying cause of the arrest is a core part of the ACLS algorithm. For pregnant patients, the differential diagnosis includes the standard H’s and T’s, plus several causes specific to pregnancy.
Pregnancy-Specific Causes (BEAU-CHOPS mnemonic):
The resuscitation team should work through this list to identify a reversible cause while continuing resuscitation efforts.
The Cardiac Arrest in Pregnancy In-Hospital ACLS Algorithm requires a coordinated, multi-disciplinary team effort. Every member must understand their role and the unique modifications needed to save two lives. Regular training and simulation drills are the best way to ensure your team is prepared for this high-acuity, low-frequency event.
At Safety Training Seminars, we provide official American Heart Association (AHA) courses, including ACLS, BLS, and PALS, that equip healthcare professionals with these lifesaving skills. Our classes cover the latest guidelines and provide hands-on practice to build your confidence. With over 70 locations across California and a commitment to excellent customer service, we make it convenient to get the training you need. To sharpen your skills and ensure you’re ready to respond effectively, book an ACLS course with us today.
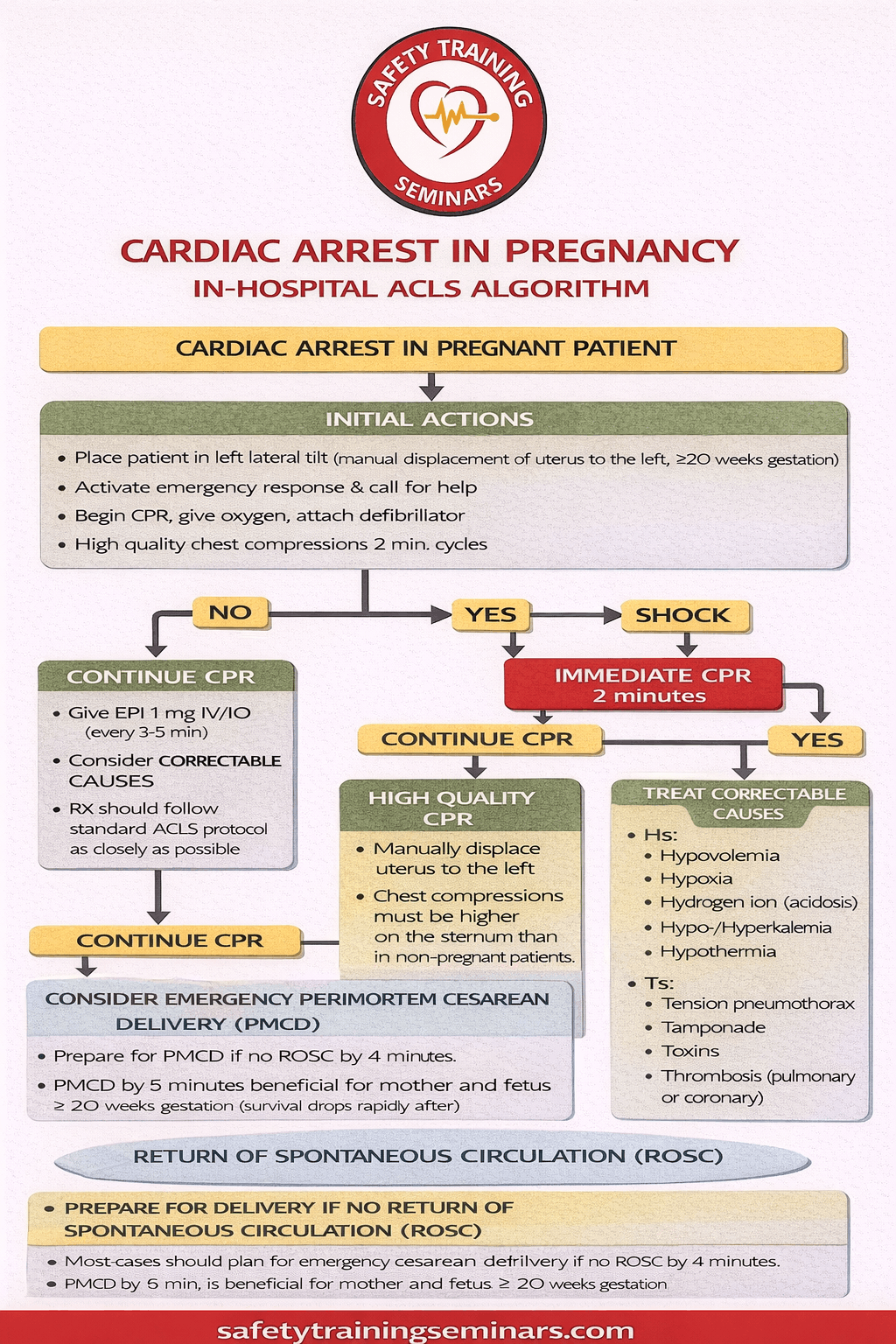
Cardiac arrest in pregnancy is a rare but life-threatening emergency that requires immediate, well-coordinated in-hospital Advanced Cardiovascular Life Support (ACLS). This infographic explains the Cardiac Arrest in Pregnancy In-Hospital ACLS Algorithm by breaking down critical actions that protect both mother and fetus. The primary goal remains high-quality maternal resuscitation, as effective circulation and oxygenation for the mother are the best way to support fetal survival. Early recognition, rapid team activation, and strict adherence to ACLS protocols form the foundation of a successful response in hospital settings.
The algorithm highlights essential pregnancy-specific modifications to standard ACLS. These include manual left uterine displacement to relieve aortocaval compression, maintaining effective chest compressions, and early airway management with 100% oxygen. Defibrillation is performed at standard energy levels and should never be delayed due to pregnancy. The infographic also emphasizes identifying and treating reversible causes, commonly summarized as the “Hs and Ts,” such as hypoxia, hemorrhage, thromboembolism, or drug toxicity, which are particularly relevant in pregnant patients.
A critical component of the in-hospital ACLS algorithm is the consideration of perimortem cesarean delivery. If return of spontaneous circulation (ROSC) is not achieved within four minutes and the pregnancy is estimated at 20 weeks or more, the algorithm recommends initiating cesarean delivery by five minutes. This intervention improves maternal resuscitation outcomes by reducing physiological stress and may also improve neonatal survival. Safety Training Seminars presents this infographic to help healthcare professionals quickly understand, recall, and apply evidence-based ACLS steps during high-stress maternal cardiac emergencies.
This algorithm adapts standard ACLS for pregnant patients. It includes maternal resuscitation, left uterine displacement, and perimortem cesarean considerations. Safety Training Seminars teaches pregnancy-specific emergency care.
CPR includes left uterine displacement to relieve aortocaval compression. Chest compressions remain standard, and monitoring maternal-fetal status is critical for survival.
If ROSC is not achieved within 4 minutes of cardiac arrest, a perimortem cesarean should be performed immediately. This maximizes survival for both mother and baby.
Epinephrine and other standard ACLS drugs can be used with caution. Maternal survival is prioritized, while considering fetal effects.
Obstetric staff, nurses, and emergency providers benefit most. Training ensures readiness for maternal-fetal emergencies. Safety Training Seminars offers expert ACLS pregnancy courses.