

Safety Training Seminars

The Pediatric Septic Shock Algorithm based on AHA 2025 Guidelines provides a step-by-step framework for early recognition, rapid fluid resuscitation, vasoactive support, and continuous hemodynamic monitoring. Learn evidence-based interventions and updated pediatric dosing protocols to improve survival, prevent organ dysfunction, and optimize outcomes in critically ill children.
Pediatric septic shock demands immediate, systematic intervention. Every minute counts when a child’s cardiovascular system fails due to severe infection. Healthcare providers need a clear, evidence-based algorithm to navigate this life-threatening emergency effectively.
The pediatric septic shock algorithm provides a structured approach to recognition, initial stabilization, and ongoing management. This systematic framework helps medical teams deliver consistent, high-quality care during critical moments when children face overwhelming infection and cardiovascular collapse.
Understanding this algorithm isn’t just about memorizing steps—it’s about saving lives. When septic shock strikes, having a clear roadmap can mean the difference between recovery and devastating outcomes for pediatric patients.
Septic shock occurs when severe infection triggers widespread inflammation, leading to dangerous drops in blood pressure and poor tissue perfusion. In children, this condition progresses rapidly and requires immediate recognition.
Key signs include altered mental status, decreased urine output, poor capillary refill, and hypotension. Unlike adults, children often maintain normal blood pressure until late in the process, making early recognition challenging but crucial.
The condition affects approximately 42,000 children annually in the United States. Early intervention within the first hour significantly improves survival rates, highlighting the importance of rapid, systematic response protocols.
The pediatric septic shock algorithm begins with rapid assessment and recognition. Healthcare providers must quickly identify signs of systemic infection combined with cardiovascular compromise.
Look for fever or hypothermia, altered mental status, and signs of poor perfusion. Children may present with tachycardia, prolonged capillary refill (>2 seconds), and decreased urine output. Hypotension is a late sign in pediatric patients.
Assess for potential infection sources including respiratory, gastrointestinal, genitourinary, or central nervous system origins. Recent antibiotic use, immunocompromised status, or chronic medical conditions increase risk.
Age-specific vital sign ranges are critical for accurate assessment. What appears normal for an adult may indicate significant compromise in a child. Use pediatric early warning scores when available to standardize recognition.
Once septic shock is suspected, immediate stabilization follows a systematic approach focusing on airway, breathing, circulation, and disability assessment.
Ensure patent airway and adequate ventilation. Children in septic shock may develop respiratory failure due to increased metabolic demands or direct lung injury. Provide supplemental oxygen to maintain saturations above 94%.
Consider early intubation if the child shows signs of respiratory distress, altered mental status, or inability to protect the airway. Positive pressure ventilation may worsen hypotension, so prepare for additional fluid resuscitation.
Establish immediate vascular access, preferably two large-bore peripheral IVs. If peripheral access fails after two attempts or 90 seconds, consider intraosseous access for immediate fluid and medication administration.
Begin aggressive fluid resuscitation with isotonic crystalloids. Administer 20 mL/kg boluses rapidly, reassessing after each bolus. Children may require 40-60 mL/kg or more in the first hour, significantly more than adult protocols.
The pediatric septic shock algorithm includes specific medication guidelines when fluid resuscitation alone proves insufficient.
Administer broad-spectrum antibiotics within the first hour, ideally within 30 minutes of recognition. Choose antibiotics based on likely pathogens, patient age, and local resistance patterns.
Common first-line choices include ceftriaxone plus vancomycin for community-acquired infections, or broader coverage like piperacillin-tazobactam for healthcare-associated cases. Adjust based on culture results when available.
When fluid resuscitation fails to restore adequate perfusion, initiate vasoactive support. Dopamine or epinephrine are first-line agents in pediatric septic shock, with dosing based on patient weight and clinical response.
Start dopamine at 5-10 mcg/kg/min, titrating up to 20 mcg/kg/min as needed. If maximum dopamine doses prove insufficient, add epinephrine starting at 0.05-0.1 mcg/kg/min. Monitor for arrhythmias and adjust accordingly.
Refractory septic shock requires additional interventions beyond initial stabilization. This phase involves more complex decision-making and specialized treatments.
Consider hydrocortisone for children with fluid and catecholamine-resistant shock. Dosing typically ranges from 1-2 mg/kg every 6 hours, though optimal dosing remains debated in pediatric literature.
Monitor for hyperglycemia and other steroid-related complications. The decision to use steroids should involve pediatric intensive care specialists when possible.
Implement continuous monitoring including arterial blood pressure, central venous pressure if central access is available, and frequent laboratory assessments. Track lactate levels, which correlate with tissue perfusion and prognosis.
Consider placement of urinary catheter to monitor output, aiming for >1 mL/kg/hr in children. Temperature management is important, as hyperthermia increases metabolic demands.
Successful implementation of the pediatric septic shock algorithm requires ongoing education and system improvements. Regular simulation training helps maintain team readiness and identifies areas for improvement.
Effective septic shock management requires coordinated team effort. Nurses, physicians, respiratory therapists, and pharmacists must work together seamlessly. Clear communication and role definition prevent delays and confusion.
Regular debriefing after septic shock cases helps identify successes and opportunities for improvement. This process strengthens team performance and patient outcomes over time.
Accurate documentation supports quality improvement efforts and helps track adherence to evidence-based protocols. Record timing of interventions, fluid volumes administered, and patient responses to guide future care decisions.
Mastering the pediatric septic shock algorithm requires more than reading guidelines—it demands hands-on training and regular practice. Healthcare teams benefit significantly from structured educational programs that combine theoretical knowledge with practical skills training.
We at Safety Training Seminars understand the critical importance of pediatric emergency preparedness. Our PALS (Pediatric Advanced Life Support) certification courses provide comprehensive training in pediatric septic shock management and other life-threatening emergencies. Through American Heart Association-certified instruction, healthcare professionals develop the confidence and competence needed to implement these algorithms effectively.
Our program covers systematic approaches to pediatric emergencies, including detailed septic shock protocols, hands-on practice with pediatric scenarios, and team-based simulation exercises. With over 70 locations throughout California and convenient online components, we make it easy for healthcare teams to maintain their emergency response skills.
The investment in proper training pays dividends when facing real pediatric emergencies. Contact Safety Training Seminars today to schedule PALS certification for your team and ensure readiness when children’s lives depend on immediate, expert intervention.
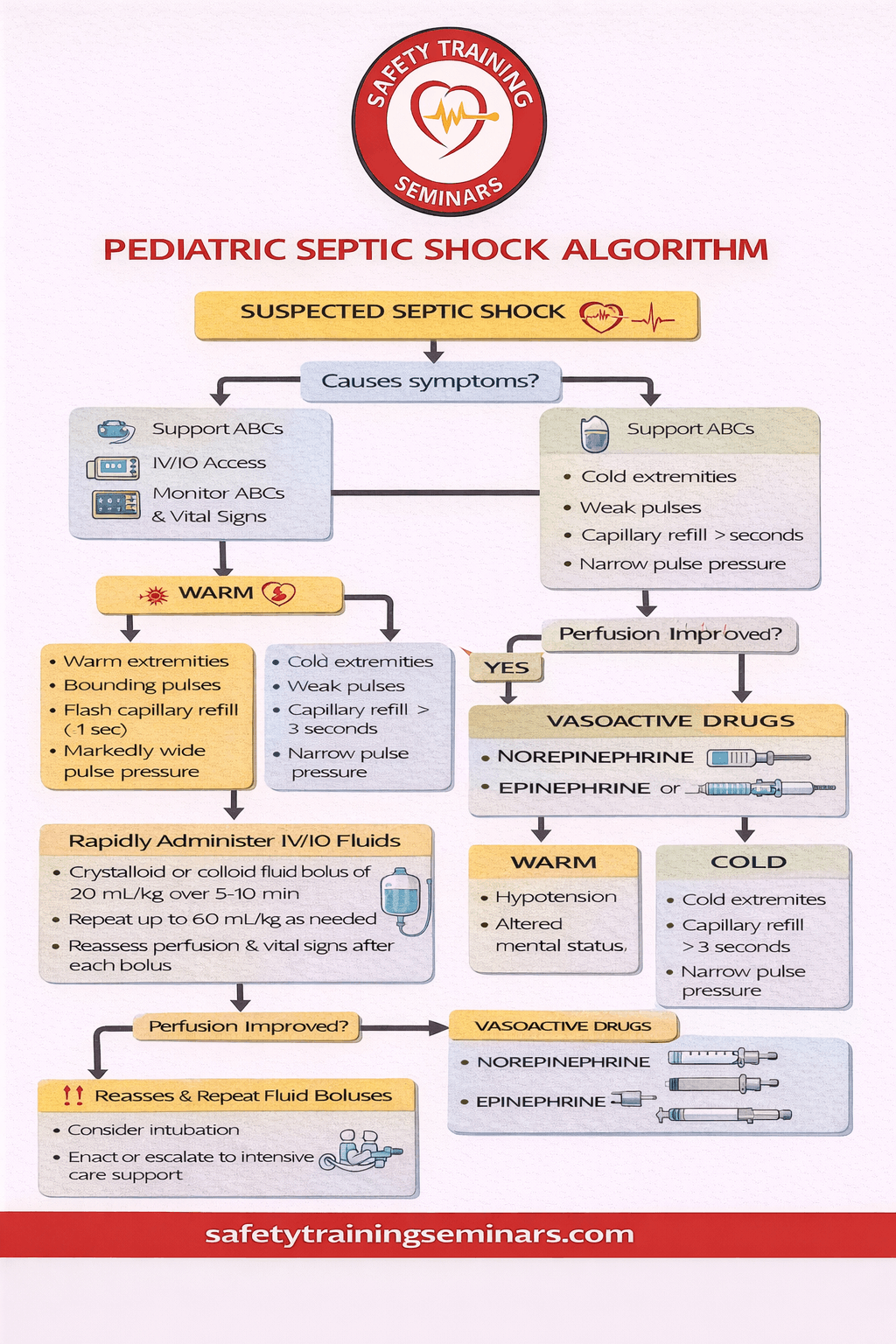
The Pediatric Septic Shock Algorithm is a critical framework designed to guide healthcare professionals in the rapid recognition and management of septic shock in children. Early identification is essential, as pediatric patients often deteriorate faster than adults due to their limited physiological reserves. This algorithm emphasizes timely assessment of vital signs, perfusion status, and organ function, allowing clinicians to initiate interventions promptly. By following a structured, evidence-based pathway, healthcare teams can prioritize lifesaving actions such as fluid resuscitation, antibiotic administration, and hemodynamic support, significantly improving survival rates.
Central to the algorithm is a stepwise approach that integrates clinical evaluation with immediate therapeutic measures. Initial steps focus on airway management, oxygen supplementation, and rapid vascular access for fluid boluses. Subsequent stages guide the administration of vasoactive agents if hypotension persists, alongside continuous monitoring of blood pressure, lactate levels, and urine output. The infographic visually represents these sequential interventions, highlighting decision points and critical thresholds that ensure timely escalation of care. This visual format simplifies complex clinical pathways, making it easier for practitioners to remember and implement best practices during high-pressure scenarios.
Additionally, the Pediatric Septic Shock Algorithm underscores the importance of multidisciplinary collaboration, including nurses, pediatric intensivists, and emergency personnel. Real-time communication, frequent reassessment, and adherence to protocolized steps reduce the risk of complications and optimize outcomes. By translating these principles into an intuitive infographic, our educational resource at Safety Training Seminars empowers healthcare providers to act decisively, ensuring prompt recognition, effective treatment, and improved pediatric patient survival in septic shock emergencies.
The pediatric septic shock algorithm is a clinical guideline designed to help healthcare providers recognize and manage septic shock in children. It emphasizes early fluid resuscitation, rapid antibiotic therapy, and the use of vasopressors to improve survival and prevent organ failure.
Septic shock is identified through persistent hypotension, poor perfusion, altered mental status, and signs of organ dysfunction. Vital signs, capillary refill, and laboratory markers such as lactate levels are used to guide diagnosis and early intervention.
Initial treatment includes rapid IV fluid administration, early broad-spectrum antibiotics, and, if necessary, vasoactive medications. Timely interventions following the algorithm are critical to stabilizing the child and preventing progression to multi-organ failure.
Continuous monitoring is recommended, with vital signs and perfusion assessed every 5–15 minutes during initial resuscitation. This allows healthcare providers to adjust fluids, medications, and other interventions in real-time.
Yes, the algorithm is structured to be used by all trained healthcare professionals, including nurses and paramedics. Proper training ensures rapid, standardized care and reduces delays in administering life-saving interventions.